The sternum is a fractured bone after a median sternotomy, like any other fractured bone.
The heart is protected behind the breast bone called the sternum, which must be cut open if heart surgery is needed so the surgeons can get access. This procedure is referred to as a median sternotomy and is still the most commonly used access method for heart surgery.
After the procedure, the sternum is positioned back together most often with stainless steel wires. Other fixation tools available are sternal bands, cables, clamps or rigid plate fixation.

Essentially the sternum is a fractured bone after a median sternotomy, and it needs to heal like any other fractured bone in the body.
The healing process involves 4 stages:
Stage 1:The Inflammatory stage with swelling of clotted blood - lasts about 1 to 2 weeks.
Stage 2:
Formation of soft callus over the next couple of weeks.
Stage 3:
Hard callus formation, usually from 4 to 16 weeks after surgery.
Stage 4:
Remodeling from week 17, - 4 months postoperatively.
Causes for potential delayed healing.
The time frames per stage depend on whether the patients have healthy bones. Each stage may be longer for patients with conditions like diabetes, obesity, high age, osteoporosis, and smokers. In addition, patients that have limited blood supply to the sternum area after an internal mammary artery harvest may have delayed bone healing. Patients diet and certain drugs like steroids and non-steroidal anti-inflammatory drugs can have an impact on bone healing too.
Healthy healing is dependent on a careful surgical alignment of the sternum, type of sternal fixation used, and continuity of bone apposition in the postoperative period. Micromotion between two bone segments has been shown to promote bone healing. However, movement more than 2 mm can result in delayed healing, a critical-sized gap, and non-union [1-2]. Rigid fixation can prevent excessive motion, however, it can not be used in all patients, e.g. patients with osteoporosis, lower bone mass, elderly and many women after menopause.
The healing of the breastbone is usually the slowest part of the recovery process after heart surgery. While the skin incision and soft tissue over the sternum visibly heal within 3-4 weeks, the healing of the breast bone takes much longer. The healing progress of the sternum cannot be followed by the naked eye, which may tempt patients to begin strenuous activities before the bone is strong enough. If patients do not follow the instructions for postoperative recovery and begin work or initiate other activities sooner than recommended, healing may be delayed considerably.
Sternal non-union and instability.
The sternum grows back together without complications in the majority of cases. Sternal wound complications such as deep sternal wound infections, superficial wound infections, sternal dehiscence, and non-union are present in 1% to 4% of patients after median sternotomy [3] which cause delayed healing and a significant increase in costs.
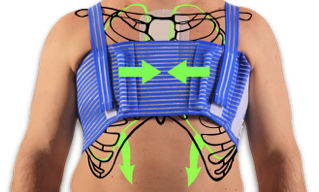
External chest stabilization is an important adjunctive treatment during the entire healing period after surgery. The chest expands during breathing, and more during coughing, sneezing or straining. If the chest is not supported from the outside, the constant chest wall movements and intermittent increase in internal pressure when coughing etc. may loosen the internal sternum fixation over time and result in incomplete healing of the sternum bone.
Incomplete healing of the sternum is referred to as sternal non-union and instability. Sternal non-union has an incidence of less than 1% [4], still - it prolongs healing much more than other complications. Having a non-union sternum or unstable chest wall can be painful or uncomfortable for the patient. If the condition is not given medical care it can result in possible infection, continued pain, and a persistent delay in the healing of the sternum.
Until medical attention can be given, external stabilization of the chest wall with dedicated chest support can relieve the symptoms associated with sternal nonunion [5].
What are the symptoms of a non-union?

The symptoms of improper healing of the sternum usually appear as pain when patients are active in their daily tasks, like reaching out or lifting something, getting up from a chair, or rolling over in bed. The sternum halves may be popping or grinding together during such movements, and there may be a clicking or clunking sensation as well as an unstable feeling in the chest. In addition, the rib cage may move irregularly when breathing. Non-union can co-occur with or without infection and may occur with or without sternal dehiscence. Sternal non-union without infection is referred to as a sterile non-union and defined as sternal pain with clicking, instability, or both for more than 6 months.
Treatment of sternal non-union
When possible a sternal non-union requires surgical intervention for a secondary sternal fixation and stabilization procedure and/or bone grafting. However, there may be patient conditions that are deemed too risky to perform another surgery, or individual patients may reject this option.
Fortunately, external chest support can be an alternative pragmatic and inexpensive option which can give these patients instant pain relief and functionality in their daily activities. This was described in a publication where constant use in 2 years resulting in the healing of the sternum [5]. A patient-reported pain, clicking and excessive movement of the sternum with everyday tasks 4 months after the third open-heart surgery. The patient also felt a ‘loud crunching sound’ and pain when attempting to lift a moderately heavy object. Instead of a 4th surgery, the patient was prescribed to use the QualiBreath sternum and thorax support. This immediately reduced pain significantly, increased activity, made uninterrupted sleep possible and improved confidence in completing everyday tasks.
After 2 years use day and night, ultrasound imaging showed the sternal edges were linked by extensive connective tissue like a ‘railway track’ forming a fibrous union between the two sternal halves. It was concluded that the QualiBreath stabilization of the sternum helped it growing this connective tissue. When considering external chest supports as a conservative treatment for long term usage in non-union patients, it is important to know there are considerable differences in the design of devices that can have a significant effect on the success.

- Does it constantly stabilize the sternum?
- Does it relieve pain?
- Does it ease breathing?
- Can it improve patient function and ease activities and exercise?
- Is it comfortable to wear 24/7?
- Is it comfortable to sleep with?
- Is it discreet to wear?
- Is it easy to wash and quick to dry?
The answer must be YES to all these factors so patients can function and go about with their daily activities and enjoy as normal a life as possible. The design and choice of material of the QualiBreath sternum and thorax support make it ideal to help non-union patients. Check out what patients, in general, say about QualiBreath here www.qualiteam.com
References:
- Claes L, Augat P, Suger G, Wilke HJ. Influence of Size and Stability of the Osteotomy Gap on the Success of Fracture Healing. J Orthop Res.1997 Jul;15(4):577-84. doi: 10.1002/jor.1100150414
- Yamaji T, Ando K, Wolf S, Augat P, Claes L. The Effect of Micromovement on Callus Formation. J Orthop Sci. 2001;6(6):571-5. doi: 10.1007/s007760100014.
- Lazar HL, Salm TV, Engelman R, et al. Prevention and management of sternal wound infections. J Thorac Cardiovasc Surg 2016; 152:962.
- Wu LC, Renucci JD, Song DH. Sternal Nonunion: A Review of Current Treatments and a New Method of Rigid Fixation. February 2005Annals of Plastic Surgery 54(1):55-8. DOI: 10.1097/01.sap.0000139564.37314.1f
- El-Ansary D, Aitken J, Zalucki N, Hardikar A. Clinical management and rehabilitation of persistent sternal instability. International Journal of Therapy and Rehabilitation, September 2015, Vol 22, No 9
Leave a comment: